


What's New In Surgical AI: 1/1/2023
2022 Roundup


Get your glasses of Cuvée Sir Winston Churchill ready, because it’s time to ring out 2022 and ring in 2023.
In our year-end roundup, we highlight the “best of” 2022 and the things we are most excited about for 2023.
But first, we are excited to offer you a 🪄sneak preview at a new product rollout developed by our team.
And if you’re not yet subscribed make sure to hit the button below to keep this goodness flowing.
🧩Table of Contents
🕶 Sneak Preview : An AI tool for MDs, built by MD.
🥂Best of 2022: AI hits mainstream - how has medicine kept up?
🎩Preview of 2023: Are MD’s obsolete? (Hint: no)
🕶 Sneak Preview
If there’s any audience that best understands us and our bizarre fascination with all things AI and surgery, it’s y’all. It is our privilege to reveal our first public build of 2023.
dotphrAIse converts a patient care plan in shorthand, full-note, or any other format into any document in the clinical workflow - custom information for patients, letters to other providers, summaries for billing, custom FAQs, the list goes on.
Are you tired of death-by-a-thousand-clicks that depersonalizes medicine, contributes to note bloat, and increases the staff needed to make your practice run? We hope dotphrAIse is everything that standard medical record text (“dot phrases”) should be, but isn’t.
Our aim is to develop an AI-based system which delivers $1 of value and saves 1 minute per note, per physician, per click.

Do you share our gripes with how clinical documentation works today? Join the movement.
We are still in an early release and working through the kinks. To say thanks for your patience, we’ll create a custom array of templates built from your own notes, just for you. Like your own personal AI assistant who writes as you would. And we’ll do it for your whole staff too.
Convinced? Signing up is free and takes 30 seconds:
Here is a quick, 60 second demo to wet your beaks.
🥂Best of 2022
2022 was a momentous year in artificial intelligence in general, with huge advances in the quality of generative models for text, images, video and audio. Applications to medicine and surgery have remained limited, in large part due to a lack of imagination.
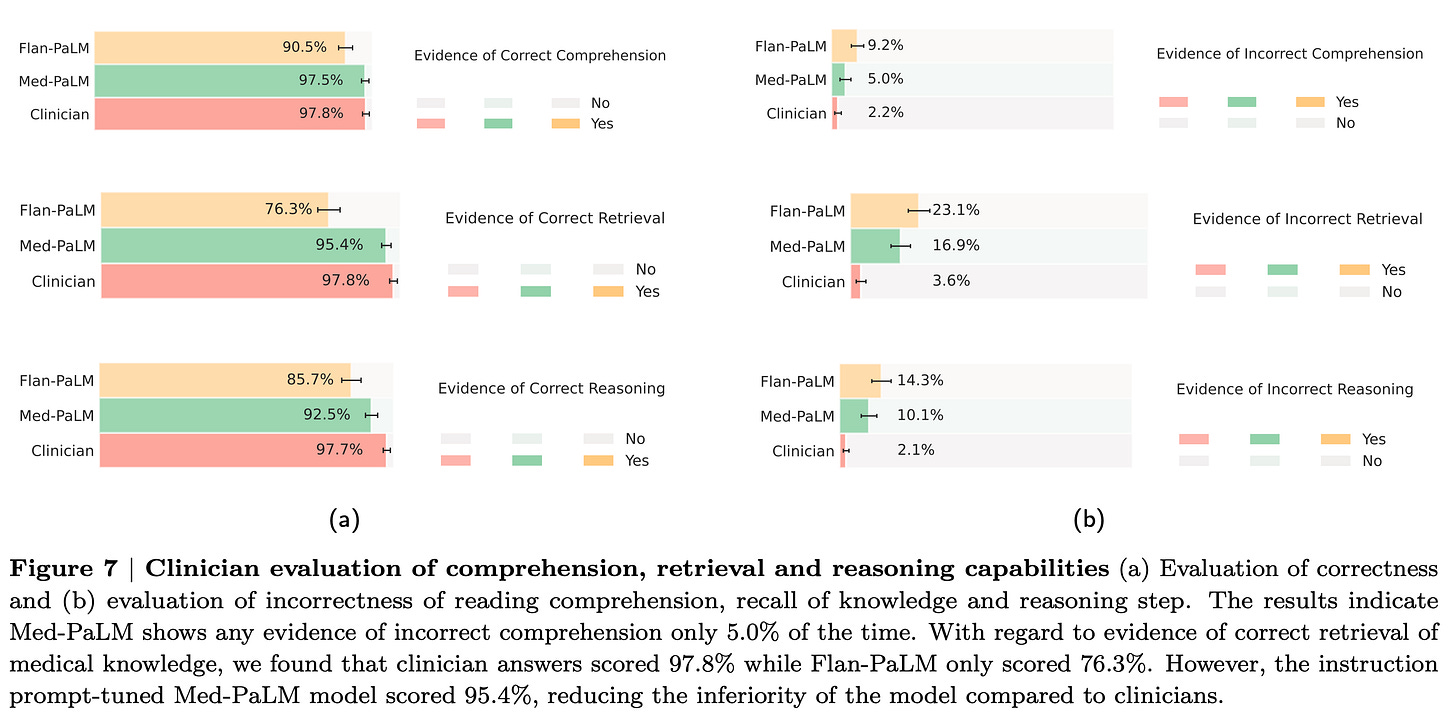
One recent Google press release paper touts their fine-tuned LLM on medical question answering (“what is the best treatment for a 34 year old man with T2DM HTN HLD A1C 8.9% never on meds”), and achieved:
USMLE multiple choice question answering 67.6% (60% is typically passing according to USMLE)
Comprehension, retrieval and reasoning capabilities slightly below humans (for now…)

This led predictably to some terrible takes (“AI is coming for your jobs” , “AI could pass the medical boards”). And there’s no way we should let this level of performance upon patients without a human-in-the-loop. But this paper is now a benchmark/new state-of-the-art (SOTA), and it is approaching closer to human expert performance, within narrow boundaries.
In order to understand where this might actually go, let’s take a brief look at other sectors. In software engineering, AI assistants are increasingly becoming integral to workflows, with some early adopters claiming they allow AI to write “80%” of their code. They view the optimal human machine interaction as machine-first, human editing. I don’t know if this is an equilibrium, or an ideal, but there’s a clear pattern happening here. (Fun fact: Dhiraj made the first prototype of dotphraise in a weekend with an AI assistant. We are fans)


The field of copywriting has already fallen to the AI
AI conquered the strategy game Diplomacy, which requires communication and coordination between players to achieve strategic goals. Using a text chat interface, AI was able to cajole, coerce and out-scheme human players. Sure, it probably cost Zuck $150M just to make this demo, but it is pretty impressive (reddit AMA with the team here)
Other professional fields are using AI to give their experts superpowers. Lexion and Harvey are two AI startups empowering lawyers to write contracts in a fraction of the time, taking care of the “boilerplate” writing for attorneys to simply review.
But there were some epic fails: see GALACTICA, the LLM trained on billions of scientific parameters, which survived less than three days before being taken down, given its propensity to create real-sounding but completely fictitious citations.

And finally, the 10x heavyweight champion of the AI world - chatGPT was released in December 2022. We devoted a whole issue to the AI assistant which has climbed above multiple groomsmen in my power ranking of friends- find our analysis and how you can use chatGPT to become better at your job, today- here.
If you haven’t used it yet, give it a whirl. We implore you to ask it to do tasks which you are fairly certain it won’t be able to do. That’s where its beauty comes out, by exceeding expectations in hard tasks.
So in summary:
LLM’s are approaching human performance in medical question answering.
LLM’s are becoming deeply integrated in computational and text-based workflows.
AI agents are increasingly able to communicate with humans and coordinate actions in service of strategic aims over time.
🎩 Looking ahead to 2023

Typically most “predictions for 2023” threads roll into inboxes around 15 December, to maximize on the hype cycle. Certainly, a fair share of “disruptors” have been plugging ChatGPT / LLMs and the generative multimodal AI landscape writ large as the innovation that will most impact 2023.
What should you be looking for in medicine and surgery x AI in 2023?
Be skeptical of the coming onslaught of journal articles with “surgery+machine learning” in the titles.
Notice that most of them are window dressing - for a variety of reasons. But start familiarizing yourself with the terms and jargon so that you can weed through the noise and identify the signal. Large language models, stable diffusion, GPT3 vs 3.5 vs 4, and some more classic ML terms will surely make its way into [insert specialty journal here] in 2023: random forests, neural networks, supervised learning, self-supervised/unsupervised learning, training/test sets, etc. Start building your dictionary, because the language is evolving every day.
We hope Ctrl-Alt-Operate can help with that - let us define things for you in a surgeon-friendly manner.
On a separate note - take a look at the author list of any major machine learning paper in the clinical sciences. There are exceptions, but in general these are engineering first-teams with physicians (or other clinicians) on board to help guide. This is an exciting opportunity for MDs - breaking down the barriers between clinicians and engineers is the opportunity I (Dhiraj) am most excited about in 2023.
Surgeons are the gatekeeper to the operating room. Without surgeon-driven engineering initiatives in AI/ML, we will still be debating how much blood was lost while other fields have fully autonomous cars and AI-assistants to do our taxes.
Be on the lookout for opportunities for human-AI teaming.
I (Dan) am putting my money where my mouth is on this one for 2023. All of the constituent pieces are there, though currently limited by expensive compute, marquee teams and gated access. All of these factors will either be exploited (paid releases) and/or eroded (open versions that are 90% as good) in the coming 12 months.
I believe the most important question of the next year in clinical medicine in surgery is HOW we team an AI agent with an MD to provide better (read: faster, safer, more accurate, more personalized) care. We may even see AI agents teamed with patients to provide higher quality interactions with doctors from the other side.
As Dhiraj highlighted above, the main limitation is no longer the technology, but the product, implementation, demonstrated efficacy within a clinical domain, and payment. That’s where we go next.
Not one single physician job will be replaced by AI.
An increasingly effective early adopter group will benefit greatly from new tools. The daily work of these enterprising radiologist, pathologists and other fields will slowly, but fundamentally, start to shift. Automating detection of medical image and text features with clinical relevance will become increasingly potent. Hopefully 2023 is the year where a packet of outside hospital records can be scanned in and a summary document generated in a matter of minutes
In the neurosurgical use case, radiologists will be increasingly supported by rapid image detection at the point of care for urgent pathology (stroke already exists, viz.ai), and pathologists will be supported by predictive genetics for tumor treatment planning.
On the text detection side, automated detection of textual data will be shown to improve hospital operations, coordination and treatment planning (prediction of length of stay and discharge, matching intensity of patient care to acuity, coordination and collaboration between specialties). One might imagine automating a consult request based on text available in the medical record to highlight key terms useful for a consultant, for example the vision exam and visual complaints scattered throughout the medical record to create an ophthalmology consultation request.
Generative AI will face continued headwinds in clinical medicine, but carefully tailored implementations will become increasingly relevant.
Medical systems will become more obviously bifurcated into the AI haves and have nots. Everyone will talk about their “data lake” but few will do the work necessary to harness the power of their resources. And to the victors will go the spoils.
It’s important to reiterate that the limiting reagent to achieving any of these aims is not technologic capability. We have methods which can do all of these with relative ease. It’s about getting the people who can see where inefficiencies are in the workflow (clinicians) in the same room with those with the data (hospital IT) those who can envision the tools for success (designers), and those who can build (engineers).
We enter 2023 as energized and excited as ever. If you are an MD hoping to get involved in this field, but don’t know how to get started, or if you’re an engineer looking to make a difference in healthcare- drop your email or reach out (ctrl.alt.operate@gmail.com). We know people ;)
Onwards!