


welcome to: ctrl-alt-operate
surgery meets AI ; vol. 1


This is Ctrl-Alt-Operate, a weekly round up of today’s quick hits from tech/ML/AI that will influence surgeons of tomorrow, plus one deeper dive charting a way for us to get there. Let’s build the surgery of tomorrow, in 5 min or less each week.
What’s the point of this?
Clinicians, have you ever felt that the technology vortex will inevitably change your practice, but don’t know how to be prepared?
Engineers, ever wondered how we can operationalize any of AI/ML innovation for the good of physicians and patients?
Maybe you’re looking for a community of like-minded surgery nerds to commiserate with about the inane use of pencil and paper rounding lists?
That’s us!
Who are you?
Dan is a pediatric neurosurgeon and faculty at Children’s National Hospital who runs a surgical data science research lab. Dhiraj is a graduating medical student entering neurosurgical training.
What do you do for fun?
We’ve published on how to turn surgical operative video into datasets built for machine learning, how to extract tangible metrics from surgical video for surgeon assessment, and more within the field of surgical data science. You can find our publications here. We are still looking for our first financial disclosures.
What should I expect?
Tweets, clinical + technical research, product reviews from the week, all in bite sized form, and a longer review at the end. Feedback always welcome. With that said, let’s get into it.
Whats 🔥📰 in👨⚕️🔪
Case List for October 21, 2022
✨ Generative AI is here ... are surgeons ready?
✏️ Erase and Replace for brain tumor resection!
🙋🏻♂️ It's getting easier and easier for MDs to use ML Generative AI is Eating Our Twitter Feed:
This chart from Sequoia has been making the rounds on Twitter. The number of companies making front-ends to interact with models like GPT-3 and DALL-E-2 is growing. Jasper just raised a round valued at $1.5B… Weirdly, none of these are healthtech.

The meme of “Generative AI” is a cute, funny f(x) to transform text (or images/video/3D render) to another. “Draw a picture of a corgi on a surfboard in the style of Jasper Johns” (using DALL-E2) … “now make it a 3D rendering” (using NeRF)… “now make it a movie” (using Meta). You get the picture.


What could a generative AI application for healthtech actually look like? How do we differentiate the “just-another-use-case” of healthtech from the actual development environment required to implement a protype and product?
The power of generative AI lies in its ability to get us 90% “of the way there” with minimal effort … or much much closer with some fine-tuning.
Lets look at education. It’s clear that the world of education will be disrupted by AI, with an arms race between AI-assistants, AI-catchers (turnitin meets Hans Niemann), and AI-innovators. So where does that leave the education of surgeons?

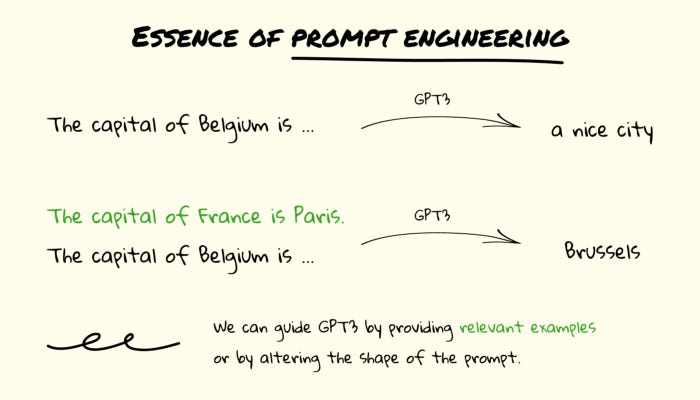
The volume of information to be ingested by trainees at every level has never been higher. If AI can answer written boards questions at expert human performance (spoiler alert: it can), prompt engineering will be solved by AI in less time than Liz Truss was in office.
This begs the question: how should we deploy this for the benefit of patients and physicians? Can we use GPT-3 and other models to help write better boards questions? Help synthesize material more efficiently? Or help learners simply be better at finding the information when they need it (Glean for surgical education?)
… side bar: Prometric bought an AI interface, so watch out- your next test might be partially written and fully graded by AI
Erase and Replace is coming for your residual tumor
Erase-and-replace was pretty mind blowing. What if we could show patients a possible post-op scan during pre-op counseling? How it their scan look with instrumentation, without the tumor, with the deformity corrected, etc. You can even use natural language description (“replace this ladybug with a bee”). So why not “replace this aneurysm with two stacked fenestrated clips” ?

Speaking of natural language…
Meta released their speech matrix dataset allowing Speech-to-speech translation with minimal annotation - their use case was a Chinese dialect called Hokkien, which has no written language.
Maybe this is a good time to bridge “patient” and “doctor” speak? Particularly in today’s world where patient’s have immediate access to charts and often see results before their providers - translating a MRI report into something a patient can digest might just prevent a frantic 10pm portal message to your clinic…
Building an AI is so easy, even a surgeon can do it?
Training models is expensive, and requires lots of compute. Until maybe now? Colossal-AI leverages commercial GPUs and fancy parallel processing to allow for large scale model development at a fraction of the computational power. this is important for healthcare - if we want personalized models which can be trained on a large, population basis, fine tuned for specific cohorts of patients, but then hyper fine-tuned on patient specific data, we’ll need to retrain models at the individual computer level.
Similarly, Replit - the browser based IDE (aka google docs for software development) - just dropped their mobile app allowing you to, quite literally, code on the go.
Now you can keep developing your health-tech startup when your first case of the day is delayed.

Feeling inspired? Drop us a line and let us know what you liked.
A Surgeon and Overwhelmed? We can add more explainers and less tech jargon.
Tech background and confused? We’ll provide more hospital/operating room context
Like all surgeons, we are always looking to get better. Send us your M&M style roastings or favorable Press-Gainey ratings by email at ctrl.alt.operate@gmail.com